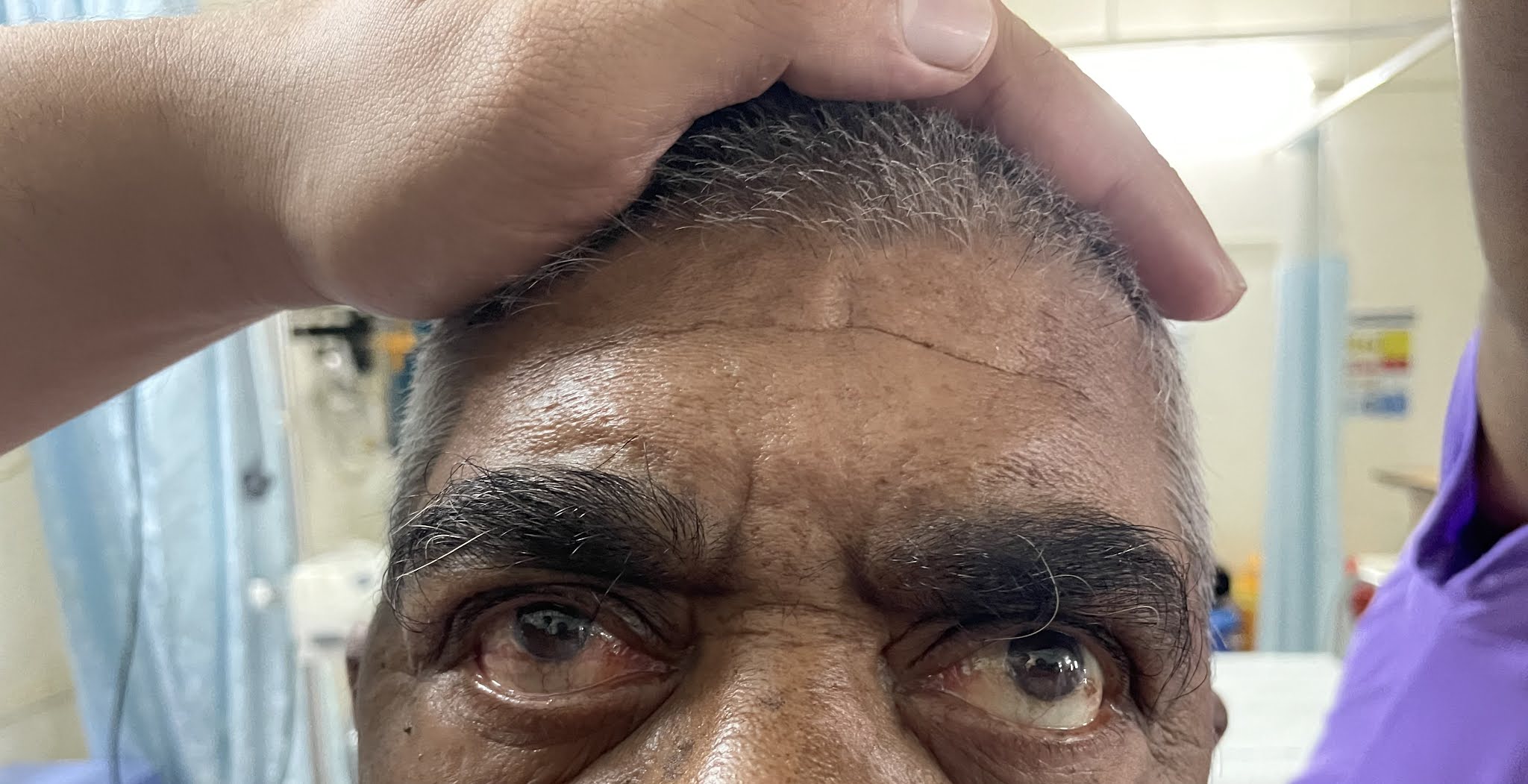
Left Facial paralysis
4th YEAR MBBS
DATE: 30/8/2021











2D ECHO 



This is an online Elog book to discuss our patient deidentified health data shared after taking his/ her guardians sign informed consent
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with n aim to solve those patient clinical problem with collect6current best evidence based input
This Elog also reflects my patient centered online learning portfolio.
Your valuable inputs on comment box is welcome
I have been given this case to solve in an attempt to understand the topic of " Patient clinical data analysis" to develop my competancy in reading and comprehending clinical data including history, clinical finding, investigations and come up with a diagnosis and treatment plan
I have further referred the case from my Senior’s elog.Thank you for the consent sir.
CASE DISCUSSION
A 74 year old patient who is a resident of Narketpalli, a retired RTC driver has come to the OPD with chief complaints of
1) Body pains since 5 days
2) Vomitings since 2 days
3) Inability in swallowing of solids and liquids since 1 day
4) Slurring of speech since today morning.
HISTORY OF PRESENTING ILLNESS
30-8-2021
The patient was apparently asymptotic 5 days back. Then he developed
Generalised Body pains of duration 5 days, insidious in onset. He took medication from Local RMP and noticed no relief
Vomitings since 4 days of about 3 to 4 episodes everyday which are non bilious, non foul smelling, non blood stained, non projectile and contained undigested food particles.
Inability to swallow both solids and liquids since 1 day
Slurred speech since today morning which was sudden in onset and he is unable to move his Lower lip.
31-8-2021
The patient is doing fine. His body pains have reduced.
No Vomitings today
6-9-2021
The patient complains of pain of Right limb which is continuous probably a fasicular pain
He also developed right eye ulcers due to lagophthalmos
Discharged today
PAST HISTORY
1)He is a known case of Diametes mellitus-2 since 25 years.
He uses Mixtard twice daily
35 units in the morning
30 units at night
2) He is a known case of Cervical spondylitis since 10 years
3) He was a known case of Tuberculosis 3 years back.
He was given 3 bags of Blood. He started ATT and developed Diminished vision and recovered after a month. He stopped ATT due to loss of hunger after a period of 5 months and again restarted the course.
Total duration of ATT- 18 months
4) He had a fall 1 year back and has been using a stick while walking thereafter
He is not a known case of Hypertension, Asthma, Epilepsy, CAD and never had undergone through any surgeries
PERSONAL HISTORY
Diet - Mixed
Appetite - Normal
Bowel and bladder movements - Regular
Sleep - Inadequate due to body pains
Addictions - None
FAMILY HISTORY - Not significant
GENERAL EXAMINATION
The patient was conscious, coherent, Cooperative and well oriented to time place and person
He is moderately built and nourished


Pallor - absent
Icterus - absent
Cyanosis - absent
Clubbing - absent
Edema - absent
Lymphadenopathy- absent
VITALS-
Temperature- 98.4 F
Pulse rate - 100/mm/min
Respiratory rate- 24 rpm
GRBS- 557
Spo2- 92%

SYSTEMIC EXAMINATION
CVS- S1 and S2 heard. No other murmurs heard
PA - Liver and spleen not palpable
Respiratory system- Normal vesicular breath sounds heard
CENTRAL NERVOUS SYSTEM EXAMINATION
Level of consciousness - Conscious
Speech - slurred
Memory - Immediate recent and remote memory present
Cranial nerve Examination:
1)Olfactory nerve - Perception of smell on both sides
2)Optic nerve - Counting finger positive from 6 metres
Visual field normal and colour vision is present
3)3,4,6 nerves- Pupils normal, ocular movements present, Nystagmus and Diplopoda absent
4)Trigeminal nerve- Prick and cotton wisp test positive
5)Facial nerve-
Deviation of mouth-
Frowning- present
Nasolabial fold- present
Blowing and Whistling- absent
Taste sensation- present
Corneal reflex- present
Clenching- present
NASOLABIAL FOLDS

FROWNING
CLENCHING OF TEETH

6) Vestibulo cochlear nerve-
Rinnes- positive
Weber- no lateralisation
7)Glossopharyngeal- gag reflex present
8) Spinal accessory- Shrugging of shoulders present
9) Hypoglossal nerve- no deviation of tongue
Motor examination
1)Inspection- Unable to completely extend his lower Limbs on supine position.
INCOMPLETE EXTENSION OF LOWER LIMBS

2)Palpation
a)Bulk- normal
b)Tone. Right. Left
Upper limb. Normal. Normal
Lower limb. Normal. Normal
c) Power. Right. Left
Biceps. 5/5. 5/5
Triceps. 4/5. 4/5
Extensor of leg. 4+/5. 4+/5
Flexors of leg. 4-/5. 4-/5
Extensors of hip. 5/5. 5/5
Doraiflexion of foot. 3/5. 3/5
Plantar flexion of foot. 3/5. 3/5
Extensors hallucinations longus- No movement on both sides
d)Reflexes
i )Superficial. Right. Left
Corneal +2. +2
Conjunctival +2 +2
Abdominal. +2 +2
ii )Deep. Right Left
Biceps. Hyperreflexive
Triceps Hyperreflexive
Supinator. Hyperreflexive
Knee. Hyperreflexive
Ankle Hyperreflexive
Sensory system
Superficial -fine touch, temperature, pain -present
Deep-position, vibration, crude touch, stereognosis, 2point discrimination- present
Cerebellum
Speech, nystagmus, ataxia, tremors, released reflexes absent
Coordination and gait
Finger nose test , finger finger test, heel knee test-present
Gait -dragging type
Romberg test -negative
Signs of meningeal irritation
Nuchal rigidity,kernigs and brudzinski’s sign - absent
Neck rigidity is present due to ossified posterior longitudinal ligament - cervical spondylitis.
CERVICAL SPONDYLITIS

INVESTIGATIONS

X-RAY CHEST


X RAY NECK

CT BRAIN
ECG

USG ABDOMEN
2D ECHO

OPHTHALMOLOGY CROSS CONSULTATION REPORT

Picture taken on 30-8-2021

Picture taken on 6-8-2021

PROVISIONAL DAIGNOSIS:
Left sided facial paralysis
TREATMENT:
Day 0:
1. Inj.HAI 39ml +1ml HAI @6ml/hr til grbs is <200mg/dl
2. Tab.Ecospirin
3.tab.clopidogrel
4. Atorvastatin/49mg/Po/Od
5. GRBS 1hrly
Day1
1.Tab.Ecospirin
2.tab.clopidogrel
3. Atorvastatin/49mg/Po/Od
4. Inj. HAI/SC/TID (8am--X--8pm)inform sugars to icu pg
5. Inj NPH/SC/BD
6.TAB.ULTRACET 1/2 TAB PO QID
7.INJ.TRAMADOL 1Amp in 100ml NS IV SOS
8. IVF- NS @75ml/hr
9.GRBS
Thankyou Zain Alam sir for the guidance!!



Comments
Post a Comment